Aseptic
Technique
Entering
the Theater
Entry to the theater
should be limited to the surgical team and the OT staff only.
Visitors if
allowed should conform to the same rules listed below:
• Those
that enter the theater must change, in the changing room into OT shoes and OT
suit
• Masks and caps must be worn before entering
OT and gowning
• All these items must be available in the
changing rooms.
Theater
Rules
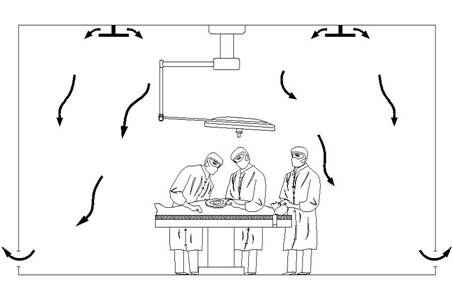
The air in the OT is
clean and filtered. This is required since surgical wounds are open to the air
in the OT.
It is desirable that the minimum number of
people should be in the operating theater, to provide safe and efficient
management of the patient. The bacteriological count in theater is related to
the number of persons and their movement in the operating room. These rules of
entry limits the infection rate.
Visitors may not be allowed to enter
restricted areas and watch the procedure from a visitors gallery
Any questions be sent to drmmkapur@gmail.com
All posts are stored in archives for access and review.
Visitors that follow may post contributions to the site.
To create consumer/provider engagement visit www.surgseminar.blogspot.com